Developmental Events:
Interaction with Dentist:
Home Oral Hygiene Routine:
Good oral hygiene removes bacteria and the leftover food particles that combine to create cavities. For infants, use a wet gauze or clean washcloth to wipe the plaque from teeth and gums. Avoid putting your child to bed with a bottle filled with anything other than water. See “Baby Bottle Tooth Decay” for more information.
For older children, brush their teeth at least twice a day. Also, watch the number of snacks containing sugar that you give your children.
The American Academy of Pediatric Dentistry recommends six month visits to the pediatric dentist beginning at your child’s first birthday. Routine visits will start your child on a lifetime of good dental health.
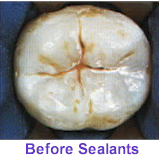
Your pediatric dentist may also recommend protective sealants or home fluoride treatments for your child. Sealants can be applied to your child’s molars to prevent decay on hard to clean surfaces.
![]()
A sealant is a clear or shaded plastic material that is applied to the chewing surfaces (grooves) of the back teeth (premolars and molars), where four out of five cavities in children are found. This sealant acts as a barrier to food, plaque and acid, thus protecting the decay-prone areas of the teeth.

![]()
Toothache: Clean the area of the affected tooth thoroughly. Rinse the mouth vigorously with warm water or use dental floss to dislodge impacted food or debris. DO NOT place aspirin on the gum or on the aching tooth. If face is swollen apply cold compresses. Take the child to a dentist.
Cut or Bitten Tongue, Lip or Cheek: Apply ice to bruised areas. If there is bleeding apply firm but gentle pressure with a gauze or cloth. If bleeding does not stop after 15 minutes or it cannot be controlled by simple pressure, take child to hospital emergency room.
Knocked Out Permanent Tooth: Find the tooth. Handle the tooth by the crown, not the root portion. You may rinse the tooth but DO NOT clean or handle the tooth unnecessarily. Inspect the tooth for fractures. If it is sound, try to reinsert it in the socket. Have the patient hold the tooth in place by biting on gauze. If you cannot reinsert the tooth, transport the tooth in a cup containing the patient’s saliva or milk. The tooth may also be carried in the patient’s mouth. The patient must see a dentist IMMEDIATELY! Time is a critical factor in saving the tooth.
![]()
Fluoride is an element, which has been shown to be beneficial to teeth. However, too little or too much fluoride can be detrimental to the teeth. Little or no fluoride will not strengthen the teeth to help them resist cavities. Excessive fluoride ingestion by preschool-aged children can lead to dental fluorosis, which is a chalky white to even brown discoloration of the permanent teeth. Many children often get more fluoride than their parents realize. Being aware of a child’s potential sources of fluoride can help parents prevent the possibility of dental fluorosis.
Some of these sources are:
Two and three-year olds may not be able to expectorate (spit out) fluoride-containing toothpaste when brushing. As a result, these youngsters may ingest an excessive amount of fluoride during tooth brushing. Toothpaste ingestion during this critical period of permanent tooth development is the greatest risk factor in the development of fluorosis.
Excessive and inappropriate intake of fluoride supplements may also contribute to fluorosis. Fluoride drops and tablets, as well as fluoride fortified vitamins should not be given to infants younger than six months of age. After that time, fluoride supplements should only be given to children after all of the sources of ingested fluoride have been accounted for and upon the recommendation of your pediatrician or pediatric dentist.
Certain foods contain high levels of fluoride, especially: powdered concentrate infant formula, soy-based infant formula, infant dry cereals, creamed spinach, and infant chicken products. Please read the label or contact the manufacturer. Some beverages also contain high levels of fluoride, especially: decaffeinated teas, white grape juices, and juice drinks manufactured in fluoridated cities. Blending the syrup, carbonation with the city water supply often makes soft drinks at fast food restaurants – so if fluoride is in the water – this is another source.
Parents can take the following steps to decrease the risk of fluorosis in their children’s teeth:
![]()
Tooth brushing is one of the most important tasks for good oral health. Many toothpastes, and/or tooth polishes, however, can damage young smiles. They contain harsh abrasives which can wear away young tooth enamel. When looking for a toothpaste for your child make sure to pick one that is recommended by the American Dental Association. These toothpastes have undergone testing to insure they are safe to use.
Remember, children should spit out toothpaste after brushing to avoid getting too much fluoride. If too much fluoride is ingested, a condition known as fluorosis can occur. If your child is too young or unable to spit out toothpaste, consider providing them with a fluoride free toothpaste, using no toothpaste, or using only a “pea size” amount of toothpaste.
![]()
Parents are often concerned about the nocturnal grinding of teeth (bruxism). Often, the first indication is the noise created by the child grinding on their teeth during sleep. Or, the parent may notice wear (teeth getting shorter) to the dentition. One theory as to the cause involves a psychological component. Stress due to a new environment, divorce, changes at school; etc. can influence a child to grind their teeth. Another theory relates to pressure in the inner ear at night. If there are pressure changes (like in an airplane during take-off and landing when people are chewing gum, etc. to equalize pressure) the child will grind by moving his jaw to relieve this pressure.
The majority of cases of pediatric bruxism do not require any treatment. If excessive wear of the teeth (attrition) is present, then a mouth guard (night guard) may be indicated. The negatives to a mouth guard are the possibility of choking if the appliance becomes dislodged during sleep and it may interfere with growth of the jaws. The positive is obvious by preventing wear to the primary dentition.
The good news is most children outgrow bruxism. The grinding gets less between the ages 6-9 and children tend to stop grinding between ages 9-12. If you suspect bruxism, discuss this with your pediatrician or pediatric dentist.
![]()


When a child begins to participate in recreational activities and organized sports, injuries can occur. A properly fitted mouth guard, or mouth protector, is an important piece of athletic gear that can help protect your child’s smile, and should be used during any activity that could result in a blow to the face or mouth.
Mouth guards help prevent broken teeth, and injuries to the lips, tongue, face or jaw. A properly fitted mouth guard will stay in place while your child is wearing it, making it easy for them to talk and breathe.
Ask your pediatric dentist about custom and store-bought mouth protectors.
![]()
You might not be surprised anymore to see people with pierced tongues, lips or cheeks, but you might be surprised to know just how dangerous these piercings can be.
There are many risks involved with oral piercings including chipped or cracked teeth, blood clots, or blood poisoning. Your mouth contains millions of bacteria, and infection is a common complication of oral piercing. Your tongue could swell large enough to close off your airway!
Common symptoms after piercing include pain, swelling, infection, an increased flow of saliva and injuries to gum tissue. Difficult-to-control bleeding or nerve damage can result if a blood vessel or nerve bundle is in the path of the needle.
So follow the advice of the American Dental Association and give your mouth a break – skip the mouth jewelry.
![]()
Tobacco in any form can jeopardize your child’s health and cause incurable damage. Teach your child about the dangers of tobacco.
Smokeless tobacco, also called spit, chew or snuff, is often used by teens who believe that it is a safe alternative to smoking cigarettes. This is an unfortunate misconception. Studies show that spit tobacco may be more addictive than smoking cigarettes and may be more difficult to quit. Teens who use it may be interested to know that one can of snuff per day delivers as much nicotine as 60 cigarettes. In as little as three to four months, smokeless tobacco use can cause periodontal disease and produce pre-cancerous lesions called leukoplakias.
If your child is a tobacco user you should watch for the following that could be early signs of oral cancer:
Because the early signs of oral cancer usually are not painful, people often ignore them. If it’s not caught in the early stages, oral cancer can require extensive, sometimes disfiguring, surgery. Even worse, it can kill.
Help your child avoid tobacco in any form. By doing so, they will avoid bringing cancer-causing chemicals in direct contact with their tongue, gums and cheek.
![]()




 Look Mom…No Cavities! / How To Raise A Cavity-Free Child
Look Mom…No Cavities! / How To Raise A Cavity-Free Child

